
A Working Menu for PTSD and Complex PTSD Care
Patricia Pop, MD · Integrative Psychiatry · Half Moon Bay, CA
If you're here, you've already done the hard part. You've figured out that what's happening to you has a shape and a name (panic showing up without warning, anxiety that lives in your body rather than your thoughts, sleep that doesn't actually restore you), and you've started getting help. That you're now looking at more than therapy isn't a failure of therapy. PTSD often needs more than therapy. Not because therapy isn't working - because PTSD lives partly in places talk doesn't always reach.
This is a menu, not a prescription. It's organized so you can find what's useful for what you're dealing with right now, and what to consider over a longer arc. Some of it has strong supporting research. Some is theory-led and clinically plausible. I'll tell you which is which as we go.
Contents
This is a long document. You don't need to read it cover to cover. Read straight through if useful, or skip to the section that addresses what you're dealing with right now. If you're in acute distress, the "Right now" section is the most immediately useful place to start.
What is trauma?
A working definition is worth establishing, because the popular understanding of trauma has shifted a lot in the last decade and the official diagnostic categories haven't fully caught up.
Trauma is what happens when an experience is too much, too fast, or too long for your nervous system to process in real time. Your mind does the protective thing: it pulls the experience out of conscious processing and compartmentalizes it. That compartmentalization is brilliant in the moment - it lets you keep functioning. The problem is that the experience doesn't actually go away. It keeps running in the background, like a radio playing in the basement: you can put it down there and close the door, but it's still on, still influencing your nervous system, still shaping your reactions. Another way to think about it: trauma is the emotional echoes of the past playing into the here and now. You can keep the basement door closed - some people do for years - but it comes with consequences (symptoms, autonomic load, what we call PTSD or CPTSD).
What happened inside, not just what happened
Gabor Maté has a working definition I find useful: trauma is not just what happened to you, it's what happened inside of you as a result. Two people can go through the same external event - a car accident, a parent's illness, an assault, a job loss - and respond very differently. Genetics, age, prior history, current resources, what came before, what came after, what was available to you in the moment - all shape what happens inside.
What this means: trauma is highly individual and largely unpredictable. It also doesn't mean it's your fault. The things that determine whether something becomes traumatic happen mostly outside your conscious control.
The response matters as much as the event
Maté then pivots to something that turns out to be enormous: and who did you tell, and what was their reaction?
The way people around you responded - believed you or didn't, supported you or didn't, named what happened as real or minimized it - shapes whether the event becomes a discrete thing you can eventually process, or compounds into a deeper, longer injury. Not being believed. Not being supported. Being told it wasn't a big deal. Having institutions (workplaces, schools, families, religious communities, legal systems) side with the harmer or minimize what happened. These aren't separate from the trauma; they become part of it, and they can be the bigger part. For many people, the secondary injury (the response that wasn't there) does more damage than the original event.
This is sometimes called institutional betrayal when an organization that was supposed to protect you didn't. It has its own research literature now (Jennifer Freyd at the University of Oregon has been the major voice), and the findings are consistent: institutional betrayal compounds PTSD outcomes, often substantially.
The flip side is also true. Being believed, being held, being told what happened was real and wrong, being met by community that understood - these aren't soft, decorative things. They're among the largest protective factors we know of. One striking comparison: after the 2006 Second Lebanon War, about 1.5% of Israeli soldiers (mandatory service and reserves) were diagnosed with PTSD. In roughly the same period, around 8% of U.S. soldiers serving in Iraq and Afghanistan had PTSD diagnoses (with militaries internationally ranging from 2 to 17%). One leading hypothesis: Israeli soldiers return to a society where mandatory military service is universal, where the adult population has done some version of military experience and meets returning soldiers at a felt level of understanding. U.S. soldiers often return to a society that can't meet them where they are, where they feel alone with what they went through. Population-level numbers can't isolate the mechanism, and other variables matter (deployment patterns, return processes, reporting norms, diagnostic culture). The consistent finding across trauma research is that being known and supported by people who understand is one of the largest protective variables we have.
This is part of why healing usually happens at least partly in relationship, especially when the wound was relational. The nervous system learned that safety wasn't possible in connection; it has to learn the opposite by experiencing it. Purely individual, mind-only approaches sometimes fall short for relational trauma.
Big T and little t
The shorthand most clinicians use distinguishes "Big T" trauma (single discrete events: a car accident, an assault, a natural disaster, war, unwanted sexual contact) from "little t" trauma (chronic relational, emotional, or environmental injuries that don't fit the discrete-event frame). The DSM-5 still leans heavily on the Big T model, partly because the original PTSD research came largely from combat veterans - a predominantly white male population responding to discrete events.
The clinical reality is broader. Things that don't always get called trauma but can cause PTSD or PTSD-spectrum responses (some of these will land for you, some won't, the point is that the category is wider than the DSM suggests):
Childhood emotional neglect (a parent who was physically present but emotionally unavailable)
A parent who was critical too often
A parent with active addiction, alcoholism, or untreated mental illness
Parents' divorce or separation, especially when conflict was high or sustained
Frequent arguments or fighting in the home growing up
Hearing violence in the home even without seeing it directly - yelling, breaking things, threats from another room
Verbal abuse (yelling, name-calling, threats - "I didn't hit you" doesn't mean what happened wasn't abuse)
Chronic invalidation ("you're being too sensitive," "stop crying, it's not a big deal")
Conditional love, or love that depended on performance, behavior, achievement, or appearance
The scapegoat or "golden child" dynamic in family - persistent unequal treatment by parents
Sibling abuse
Frequent moves or chronic housing instability in childhood
Foster care, kinship care, or adoption transitions (with the disruptions in attachment and identity that come with them)
Ambiguous loss - a parent or family member who's physically present but absent in another way (dementia, severe mental illness, addiction), or a missing or estranged family member whose fate is unresolved
Bullying in school
Abuse of any kind (emotional, verbal, physical, sexual) by a teacher, coach, or other figure of authority
Being the "different" kid (queer, neurodivergent, ethnically or culturally different, gifted, disabled) in a context that didn't accept it
Hospitalization as a child (separation from caregivers, scary medical procedures, prolonged stays)
Public humiliation or shaming, especially when sustained or in front of people whose opinion mattered to you
Sustained sexual harassment or unwanted advances, including the kind with "plausible deniability" - the comments, the touches, the situations that the other person can always frame as accidental or as you misreading
Workplace bullying or harassment
Harassment or hostility from clients, patients, students, or anyone else in a working relationship where you couldn't easily leave
Online harassment, cyberstalking, doxxing, or sustained digital cruelty
An adult relationship with emotional or psychological abuse - controlling, manipulating, gaslighting, coercive - even without physical violence
Reproductive trauma (miscarriage, pregnancy loss, infertility, traumatic birth experience for parent or baby, abortion experienced as loss)
Witnessing violence rather than experiencing it directly
Medical trauma (procedures, prolonged hospitalization, hard diagnoses)
Caregiver illness in childhood (children parentified into roles too big for them)
Early death of a parent, sibling, or other close attachment figure
Death of a pet, especially when the loss wasn't acknowledged or held by people around you
Religious or spiritual abuse
Persistent racial, ethnic, or other discrimination
Immigration and refugee experiences, including forced migration, fear of deportation, and the cultural assimilation pressure that comes with them (forced or "soft" - the slow erosion of your original culture, language, or self to fit in)
Being closeted, or having to hide a core part of who you are for long periods
Cult or high-control group experiences
Financial precarity that lasted years
Growing up in chronic dysregulation, even without obvious abuse
And then there's the kind that's even smaller and repeated - "death by a thousand paper cuts." Each individual incident doesn't seem big, but the accumulation does the work over time.
I'm not fully sold on the "T versus t" shorthand (the size language can read as dismissive of the smaller things, which can do real damage). The distinction it points to is useful, though: not all trauma is event-shaped, and the smaller, more chronic kind is often the most missed.
One research note worth flagging here: the Adverse Childhood Experiences (ACE) Study, run by Felitti, Anda, and colleagues at Kaiser Permanente in the late 1990s, documented a strong dose-response relationship between childhood adversity and adult outcomes - both mental health (depression, suicidality, addiction) and physical health (heart disease, autoimmune conditions, even earlier mortality). The framework has been refined and expanded since, with additions like discrimination, housing instability, and community violence. The point isn't that ACE scores are destiny - they aren't, and many people with high scores live well - it's that the long arc from childhood adversity to adult disease is real, documented, and a reason to take all of this seriously even when the original events feel "small" or "long ago."
Where it lives
Trauma lives in places that don't respond well to talk alone:
Biologically and neurologically. The body's stress response systems get rewired toward hypervigilance. The amygdala (threat detection) becomes oversensitive. The hippocampus (context) and prefrontal cortex (regulation) get less effective at their jobs. The autonomic nervous system gets stuck in survival modes - the four Fs: fight, flight, freeze, fawn. The implicit memory of the trauma sits more in body and emotional systems than in language and narrative.
Worth holding alongside all of this: every piece of it is your body doing exactly what evolved to keep you alive. The hypervigilance was protective once. The shutdown was protective once. The fawning was a survival strategy that worked. The system isn't broken - it's overcorrected and stuck in protection mode after the threat is gone. That's not the same as you overreacting or being too much. It's a wise system applying old logic to a new situation.
Psychologically. Beliefs about self ("I should have stopped it," "I'm broken"), beliefs about others ("no one is safe"), patterns in relationships, identity, sense of agency.
Spiritually, in many traditions. Some frameworks describe trauma as a fragmentation or loss of self - parts of you that left during the experience and need to be brought back. Soul retrieval in shamanic and indigenous traditions is one expression of this. You don't have to adopt any particular belief system to find these frames useful as descriptions of an experiential reality. Many people find that the spiritual language reaches something the psychological language doesn't.
Two useful metaphors
The fire alarm. Trauma as an alarm system that got miscalibrated by going off during a real fire. It learned to detect threat at a much lower threshold than necessary, so now it goes off in safe places too - in your kitchen, in line at the grocery store, with people who love you. Treatment isn't about removing the alarm (you need an alarm). It's about recalibrating, so the alarm goes off when there's an actual fire and not when someone burns toast.
The radio in the basement. The mind compartmentalized the experience and put it somewhere it didn't have to engage with daily. The radio is still on, though. It plays into your nervous system whether you can hear it consciously or not. You can't just walk down and turn it off - if you opened the basement door without preparation, the volume would overwhelm you. Healing is partly about building enough capacity to gradually go down there with support, listen to what's playing, and slowly turn the volume down. Through repetition, not by force.
Capacity, not catharsis
A frame I've come to: the goal isn't to dump out the trauma, fling it out of you, or have one enormous breakthrough. It's to build the capacity to be with it - emotionally, somatically, relationally - without getting flung back into fight, flight, freeze, or fawn. Think of it like physical training. A support group where everyone vents about their pain can be validating and necessary, but it doesn't, on its own, build the muscle (a group of out-of-shape people talking about how their bodies feel can be supportive and human, and you still need to actually exercise to change anything). Building the muscle requires practice with the actual sensations and emotions, in titrated doses, with enough resourcing to stay regulated. That's why serious trauma work emphasizes "resourcing" before "processing."
The work isn't only being with difficult emotions, either. It's also building the capacity to feel safe in safe places - to experience peace, passion, creativity, and love. All things that, during the trauma, may have been paired with danger and got blocked off. The nervous system has to learn it's allowed those experiences again.
Why consistency matters
Trauma is held in the nervous system and in implicit memory. Neither responds well to single insights, however correct. They change through repetition. Daily nervous system practices that show the body, over and over, that it is safe here and now are how the body comes to actually believe what your mind already knows. Treatment is a long arc of small repeated experiences, not a few big breakthroughs (those happen too, but they're not the engine). A place you can go regularly - a daily practice, a weekly therapist, a monthly group - is doing real work even when it doesn't feel dramatic.
What we're working with
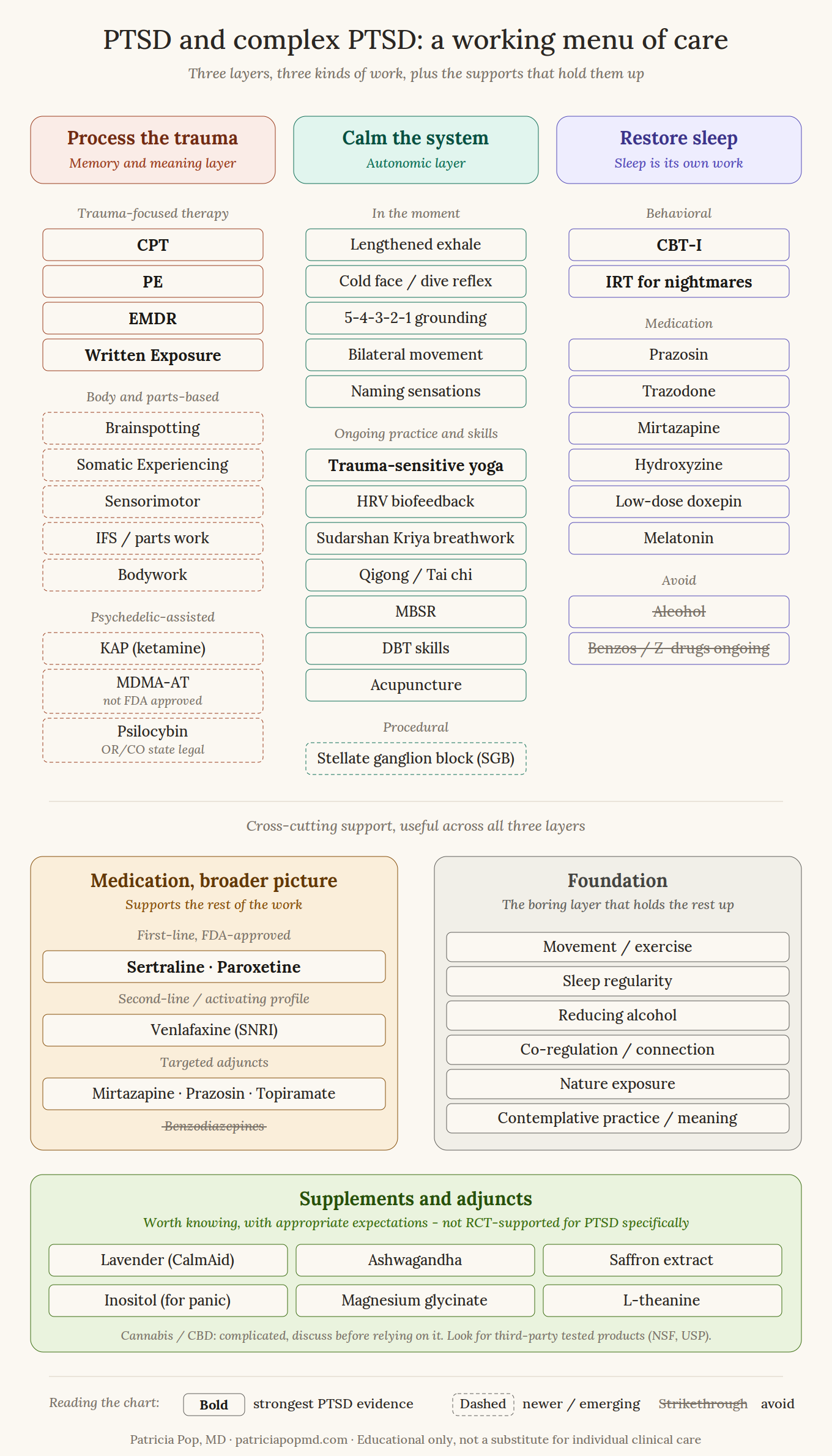
PTSD shows up in three rough layers, and different tools work on different layers. It helps to know this so you can match the tool to the layer you're trying to move.
The memory and meaning layer. The part of you that experiences the trauma as still happening, that reacts to triggers, that has shaped beliefs about yourself or the world. Trauma-focused talk therapy is well-suited to this layer.
The autonomic layer. The body's nervous system, stuck in some form of high alert (or oscillating between high alert and shutdown). This is where panic, hypervigilance, startle, reactivity, and that bracing-against-everything feeling live. Talk therapy doesn't always reach this layer reliably. Body-based and physiological approaches usually do better here.
A useful frame here is the window of tolerance (Dan Siegel's term): the range of arousal where you can think and feel and respond effectively. Above the window is hyperarousal - fight or flight, panic, racing thoughts, can't sit still. Below it is hypoarousal - freeze, shutdown, numbness, dissociation, can't feel anything. Trauma narrows the window, so smaller things bump you out of it. A lot of nervous system work is about widening the window back up so more of your daily life happens inside it instead of at the edges.
The sleep layer. Sleep sustains the other two layers and gets wrecked by them. Sleep has its own evidence-based treatments, and it's often worth treating directly rather than waiting for it to "improve when the trauma resolves." It frequently doesn't, on its own.
The menu below addresses all three layers because they sustain each other. You can start with the layer that's loudest, and progress in one usually softens the others.
PTSD or complex PTSD?
There's a distinction between PTSD (often after a discrete event or short series of events) and complex PTSD (CPTSD - typically after prolonged or developmental trauma, especially in childhood, or in chronically inescapable contexts). The ICD-11 formally recognizes CPTSD; the DSM-5 doesn't, but the clinical picture is well-documented.
CPTSD includes the core PTSD symptoms (re-experiencing, avoidance, hyperarousal) plus what's called "disturbances in self-organization":
Affect dysregulation - intense emotional reactivity, or shutdown, or oscillation between them
Persistent negative self-concept - shame, worthlessness, "something is wrong with me" as a felt sense rather than a thought
Difficulties in relationships - trust, intimacy, sustained connection
Most of this menu serves both, with some differences in emphasis in CPTSD:
Pacing matters more. Going straight to exposure-based trauma processing can destabilize someone with CPTSD. A phased approach (stabilization, then processing, then reintegration) is the standard framework.
Skills first or in parallel. Modalities like DBT skills, IFS, or STAIR often come before or alongside trauma-focused therapy.
Body and attachment. Body-based work and attention to relational and attachment patterns tend to be more central for CPTSD than for single-event PTSD.
Longer arc. Treatment is typically longer, with more layered work over time.
If your trauma history is chronic or developmental, or if you find the standard PTSD framing doesn't quite capture what's going on for you, worth bringing this up. The plan adjusts.
If you want to self-screen, the PCL-5 (PTSD Checklist for DSM-5) is a free 20-item self-report measure for PTSD; the ITQ (International Trauma Questionnaire) screens for both PTSD and ICD-11 CPTSD. Both are widely used in research and clinical settings and available freely online. Filling one out gives us a starting point - not a diagnosis, just a place to begin the conversation.
Safety first
Before everything else: if you're still in the environment or relationship that caused or is causing the trauma, deep healing doesn't really start. The nervous system can't unwind from threat while threat is ongoing. This is true for ongoing abuse, ongoing harassment, work environments that are recreating the trauma daily, relationships that are actively harmful. Treatment can help you cope, can keep you functional, can sometimes give you what you need to leave or distance yourself. The deep work - actually releasing what's compartmentalized, recalibrating the alarm - depends on two things: the environment being actually safe (in reality, not just conceptually), and your nervous system coming to feel safe in a body-knowing way (which lags the intellectual knowing, often by a lot).
This is harder than it sounds. People stay in harmful situations for real reasons: financial dependence, immigration status, children, fear of escalation, lack of alternatives. "Just leave" is a privileged sentence. If you're in that position, the first part of the work is often building the conditions that make leaving (or distancing yourself enough that you can heal) possible: resources, support network, plan, safety. Domestic violence advocates, workplace HR or attorneys, social workers, and trauma-informed therapists can all be part of that scaffolding.
Meanwhile, you're not stuck doing nothing while you build those conditions. Coping skills, resourcing, the in-the-moment tools below, building connection with people who can hold what's happening - these all count as real work and they sustain you while the bigger pieces come into place.
If you're already out: notice that part of the work is now letting your nervous system catch up to the fact that the danger is over. The body often doesn't "believe" it for a while - and I'm putting believe in quotes because this isn't a cognitive process, it's a slower body-knowing that builds through repeated safe experiences over time.
Right now: tools for this week
These won't fix PTSD. They're tools for riding panic waves and bringing your nervous system down from high alert in the moment. Worth practicing when you're calm so they're available when you're not. Calm is when you build the habit; activated is when you need it.
Lengthening the exhale. Breathe in for 4 counts, out for 6 or 8. The exhale is the parasympathetic side of the breath (the rest-and-digest side); making it longer than the inhale shifts the autonomic balance. You won't feel transcendent. You might feel a half-step calmer, which is the point.
If counting doesn't stick, a visual or tactile breath pacer can help. The Ohm Resonance Lamp (ohm.health) pulses light at resonance breathing frequency (around 5-6 breaths per minute, the rate that tends to maximize heart rate variability). Apps like Breathwrk, the Breathing app on Apple Watch, and several HRV training apps do similar things with screen visuals or wrist vibration. The point isn't the device, it's that an external pacer makes settling into the slow rhythm easier than counting alone. Useful for both daily practice and in-the-moment regulation.
Cold water on your face. Splash, hold a cold pack to your cheekbones, or briefly submerge your face in cold water. This activates the mammalian dive reflex (slowed heart rate, parasympathetic activation), which is one of the few reliably calming physiological tricks for acute panic. Brief is enough - 15 to 30 seconds.
Convergence / oculocardiac reflex. Hold a finger about a foot in front of your nose and slowly bring it toward you while keeping your eyes on it - cross your eyes, in other words - and hold the convergence for 10-20 seconds. Or do near-far focusing (focus on a fingertip close, then a far object, then back). Activates a parasympathetic reflex via the vagus nerve and the oculocardiac pathway. Odd-feeling, free, and sometimes reaches what breath doesn't.
Bilateral, rhythmic movement. Walking with attention, swimming, drumming, dance, even tapping alternating shoulders. The rhythmic alternation seems to settle activation in a way still meditation often can't. (This is part of why EMDR works for some people, though there's debate about whether the bilateral piece is actually the active ingredient.)
Bilateral sound. Free apps and YouTube tracks deliver alternating left-right audio tones. The bilateral stimulation can settle activation similarly to bilateral movement, without needing to move. Useful at night, on planes, or any time movement isn't an option. Search "bilateral stimulation audio" - many free options.
Naming sensations, not emotions. "Tightness in chest, jaw clenched, heat in face, knees weak" is more useful than "I'm anxious." Specific body words give your mind something concrete to track and signal to your nervous system that you're processing rather than spiraling. This is also good practice for therapy work; emotion labels are often summary judgments, but sensations are data.
5-4-3-2-1 grounding. Five things you can see, four you can hear, three you can touch, two you can smell, one you can taste. Familiar but it works because it pulls cognition back to present-tense sensory data when your system is replaying past or projecting threat.
If you tend to dissociate (zone out, feel unreal, lose time), pair grounding with something tactile and a little uncomfortable: a cold object, strong taste, weighted blanket pressure, an acupressure ball (the spiky kind - the small ones you can roll under your feet or hold in your hand work well). Numbing tools (substances, scrolling, sleep) tend to deepen the dissociation; sensory anchors tend to come the other direction.
These are surface tools. They don't address the underlying trauma. They buy you function while the deeper work happens.
Sequencing: what to try first
Instead of giving you a list and asking you to guess, here's how I'd think about ordering, knowing that real people don't follow tidy algorithms. It's worth reading this section before the treatment menu below, so you have a frame for how to think about choosing.
If you're still in the harmful environment: safety planning first. The deep healing work waits, but that doesn't mean nothing happens in the meantime. Coping skills, resourcing, building support networks, getting clear on what leaving (or distancing) would require - all of that is meaningful work. The in-the-moment tools in the "Right now" section apply.
If panic is interfering with daily function: stabilize autonomic load first. Acute tools (breath, cold, grounding), a daily mind-body practice, possibly medication or SGB. It's hard to do trauma processing while in chronic panic.
If sleep is wrecked: treat sleep directly. CBT-I, IRT if nightmares are prominent, address alcohol if relevant, possibly medication. It's hard to do anything on no sleep.
If you're functional but stuck in PTSD symptoms: trauma-focused psychotherapy (CPT, PE, EMDR, or written exposure) is the highest-yield move. Add medication if needed to support the work.
If you've done one or more trauma-focused therapies without resolution: options include trying a different modality (e.g., somatic if you've done cognitive, or vice versa), intensive formats (multi-day or week-long treatments), KAP, or building out the lifestyle and body layers more deliberately.
If your trauma is complex or developmental: consider a phased approach - skills first or in parallel (DBT skills, IFS, STAIR), with trauma processing layered in once stabilization is enough to sustain it. The Herman / van der Kolk / Cloitre framework: stabilization, then processing, then reintegration. Skipping ahead - going straight to exposure-based processing when stabilization isn't there - tends to flood rather than help.
If you're not in therapy yet: worth finding a trauma-trained clinician. If you have a therapist, worth asking whether their work with you is trauma-focused or something else, and what they'd recommend.
Time horizons
How long to give something before deciding it's working or it isn't:
Medication trials usually need 4-6 weeks at a therapeutic dose before you can call it.
Trauma-focused therapy typically shows meaningful shift by sessions 4-8, with a full course running 12-16+. Standard pacing is 1-2x per week; intensive formats can compress that.
Body-based work is harder to time because the markers are more felt than measured; I usually suggest a 6-8 session commitment before deciding whether to continue.
Lifestyle changes show effects in 2-4 weeks for sleep and alcohol; longer for movement and connection.
Supplements: most things at adequate doses should show some signal within 4-6 weeks.
Layering versus switching
When something is partially working, layering (adding a second modality) usually beats switching. When something isn't doing anything after a fair trial, switching is the move. When something is making things worse, stop sooner rather than later, and let me know.
When sequencing breaks down
Some situations change the order of operations:
Active substance dependence often needs concurrent treatment, not "after we settle the trauma."
Current self-harm urges, suicidal intent, or recent attempts need safety stabilization first; trauma processing comes once there's enough ground to work from.
Untreated psychotic symptoms need their own assessment and treatment before deep trauma work.
Severe dissociation that interferes with daily safety calls for stabilization-focused work (grounding skills, parts work, sensorimotor stabilization) before exposure-based trauma processing.
None of these mean "you can't do this work." They mean we sequence carefully and don't skip steps.
Treatment to consider
This section is about the actual work of treating PTSD - not symptom relief but resolution. Several routes exist; the right one depends on what you've tried, what fits, and what's accessible.
Trauma-focused psychotherapy
The strongest-evidence treatments for PTSD are the trauma-focused therapies, meaning they directly address the traumatic memory rather than working around it.
Cognitive Processing Therapy (CPT). Structured, around 12 sessions, focuses on the meaning you've made of the trauma (the "stuck points" - beliefs about why it happened, what it says about you, what it says about the world). Solid evidence base. Doesn't require detailed retelling of the trauma.
Prolonged Exposure (PE). Repeated, controlled engagement with the trauma memory and with situations you've been avoiding. Effective, but harder to sit through. Not for everyone, and not for every stage.
EMDR. Uses bilateral stimulation (eye movements, taps, sounds) while you process the trauma. Effective; the mechanism is still debated. Often feels gentler than PE for the people it suits.
Written Exposure Therapy. Five sessions of structured trauma writing. Newer, evidence is good, underused. Worth knowing about if the idea of weekly talk-based sessions feels like too much.
If you're in therapy, worth asking what modality your therapist is using. Many therapists treat trauma without using a structured trauma-focused protocol, which can help in other ways - relationship, stabilization, broader life processing - but doesn't always resolve PTSD symptoms reliably on its own. If you haven't done a structured trauma-focused therapy, that's often the highest-yield move available - either as a focus within your existing therapy or with an additional clinician for the protocol-specific work.
A note on dose and pacing: standard weekly therapy (1-2x per week) is the most common rhythm, and 1-2x per week is usually about right for trauma-focused work. Less than weekly often makes it hard to build and hold the processing thread. Intensive formats exist too - multi-day, week-long, or month-long protocols (Emory's intensive PE program is a known example) - and can be valuable when life logistics make weekly hard or when the work needs concentrated attention. There's no single right pacing; the principle is enough frequency to maintain momentum.
Body-aware psychotherapy
Talk therapy with a strong body-awareness focus - the clinician helps you notice and track what's happening in your body as you engage with the material. Often useful when traditional talk therapy has missed the body's part of the story, or when the trauma sits in places words can't quite reach.
Brainspotting. A newer approach where the practitioner helps you find a "gazespot" related to activation in your body, and held attention to that point seems to allow processing. I think of Brainspotting (along with practices like trance work, shamanic journeying, and holotropic breathwork) as something close to "psychedelics sober." The essential format is the same: mindful presence with what's coming up in heart, mind, and body, following the flow of your own inner wisdom, with an attuned relational presence guiding you. The work happens largely subcortically - below conscious cognition - which is part of why it can reach material that talk-based approaches can't. In my view, it distills what's already working in the best therapy offices and makes it more explicit. I trained in it and use it in practice. The research base is thinner than CPT or PE because it's newer and harder to study in standard RCT designs - and I see it help people regularly, sometimes more than talk-based approaches, especially for people who get stuck in talk or who can't access the trauma through words.
Somatic Experiencing, Sensorimotor Psychotherapy. Body-tracking approaches developed by Peter Levine and Pat Ogden respectively. Both are talk therapy with a strong body-awareness focus - the clinician helps you notice and track what's happening in your body as you engage with the material. The research base is still developing, which doesn't mean they don't work. They help a lot of people, particularly when talk-based approaches haven't reached the body's part of the story.
Body-based practices and procedures
More direct work with the body - through movement, physical contact, breath, nervous system training, or in-the-body practices that develop autonomic regulation. Often most useful when the body is loud and the mind is already saturated with insight.
Bodywork (trauma-informed). Different from Somatic Experiencing or Sensorimotor (which are talk therapy with body awareness): bodywork involves hands-on physical contact or movement-based work. Trauma-informed massage, craniosacral therapy, myofascial release, Feldenkrais, Alexander Technique, TRE (Tension and Trauma Releasing Exercises). Useful as adjuncts. One important caveat: body memories and strong emotional responses can surface during bodywork, so working with a trauma-informed practitioner who can hold what comes up matters more than the specific modality. Not typically a primary trauma treatment on its own, but valuable for the body layer.
Trauma-sensitive yoga. Has RCT evidence (van der Kolk and colleagues, 2014) for women with chronic treatment-resistant PTSD. Important caveat: this is the specifically adapted form, not a regular yoga class. The trauma-sensitive elements (predictability, choice, no hands-on adjustments without explicit consent, gentle attention to interoception, no shaming or pushing) are what makes it different.
If you can't find a specifically trauma-sensitive class in your area, you can ask any yoga teacher about how they handle these elements: do they offer modifications without making it weird, do they avoid touching students without explicit consent, do they invite (rather than command) the practice. Style names that tend to work better for trauma: yin, restorative, gentle hatha, slow flow, sometimes therapeutic or chair yoga. Styles to be careful with: power yoga, hot yoga, very fast vinyasa, anything marketed as intense or as a workout - not because they're bad, but because the intensity can be activating in ways that don't help when you're already in autonomic overload. The right class should feel like coming home to your body, not like another arena where you have to perform.
HRV biofeedback. Training your heart rate variability through slow guided breathing while you watch your physiological response in real time. Solid evidence base for anxiety, some PTSD evidence, and concrete enough that it doesn't require believing in anything.
Acupuncture. Has been studied for PTSD with a growing evidence base. Hollifield and colleagues have run multiple trials over the past two decades: their 2007 pilot showed acupuncture was equivalent to group CBT and superior to a waitlist for PTSD symptoms; their 2024 RCT in 93 combat veterans (JAMA Network Open) showed verum acupuncture outperformed sham on clinician-rated PTSD symptoms and on fear extinction physiology. Engel and colleagues' 2014 effectiveness trial in active-duty service members also showed positive outcomes when acupuncture was added to standard PTSD care.
Worth knowing about: the NADA protocol (National Acupuncture Detoxification Association) is a specific 5-point auricular (ear) protocol originally developed for addiction treatment, now widely used in trauma, addiction, and disaster relief. It's delivered in group format, 30 to 45 minutes, no talking required - everyone sits together and receives the same 5-needle ear treatment. Community acupuncture clinics in many cities offer sliding-scale rates and NADA-style group sessions, which makes this one of the most accessible body-based options on the menu.
Acupuncture outside the NADA protocol can also be effective - a skilled practitioner will use diagnostic principles from traditional Chinese medicine to choose points specific to your presentation. People often report feeling more able to sink into a felt sense of safety after sessions, or describe a sense of "release" - emotional, somatic, or both - during or after the work.
Acupuncture works primarily on the autonomic layer (stress response, sleep, hyperarousal). Less likely to be a standalone treatment for the memory and meaning layer. Generally well-tolerated; very low-risk in trained hands.
Equine-assisted therapy. Working with horses has emerged as an option, particularly for people drawn to animals or those who feel stuck in talk-based therapy. The proposed mechanism: horses are large prey animals exquisitely sensitive to nervous system state, so working with them both requires and develops the regulated, embodied presence trauma recovery is trying to build. The relationship offers co-regulation, non-verbal processing, and real-time sensorimotor feedback.
Evidence is preliminary and mixed. Johnson et al.'s 2018 randomized trial of therapeutic horsemanship in veterans showed significant PTSD symptom reductions. Arnon and colleagues developed a manualized 8-session protocol (EAT-PTSD); their 2021 open trial showed good feasibility and about 50% of veterans achieving clinically significant improvement, with notably low dropout (meaningful given that PTSD treatment dropout rates in veterans often run 30 to 40%). A 2025 multi-site observational study of the EAGALA model in 107 veterans showed pre-to-post improvements in PTSD, depression, and life satisfaction. Several smaller studies have been mixed - some positive, some not statistically significant, though most trending in the right direction.
Two formal models to know about: EAGALA (Equine Assisted Growth and Learning Association) and PATH International (Professional Association of Therapeutic Horsemanship International). Both certify programs and offer practitioner directories. Many programs have specific veteran funding; civilian access varies by region.
Honest framing: not a first-line treatment, but a real option, particularly if other approaches haven't engaged you or if you have a pull toward animal-based work.
A note on framing: the "polyvagal" model (Stephen Porges) shows up everywhere in trauma circles. The clinical idea - that we have different autonomic states, and that safety and connection regulate them - is useful and matches what people experience. The neurophysiological claims behind the model are debated among researchers. The practices built on it can still help; the framing is a useful clinical map, even if the underlying biology turns out to be more complicated than the popular version suggests.
Skills-based and parts-based approaches
Especially relevant when emotion regulation is hard, when shame or self-criticism is loud, or when the trauma picture is complex.
IFS (Internal Family Systems) / parts work. Approaches trauma by working with the different "parts" of the self that hold different aspects of experience (the protector, the wounded one, the inner critic, etc.). Increasingly well-supported clinically, with growing research evidence. Particularly useful when shame, self-criticism, or fragmented sense of self are prominent. Maps interestingly onto older spiritual frames of soul fragmentation, though the language and structure are different.
DBT (Dialectical Behavior Therapy) skills training. A structured skills package for emotion regulation, distress tolerance, mindfulness, and interpersonal effectiveness. Not trauma-focused on its own; the skills support the rest of trauma work, especially when affect dysregulation is significant. Available as full programs or skills-only groups.
STAIR (Skills Training in Affective and Interpersonal Regulation). Marylene Cloitre's protocol, explicitly designed as a precursor to trauma-focused therapy for CPTSD. Eight skills sessions before sixteen narrative-processing sessions. Less widely available, worth asking about if you can find a STAIR-trained clinician.
Mindfulness practices like RAIN and self-compassion. Two practices that emerged from Buddhist contemplative traditions but are accessible without requiring commitment to any particular ideology, belief system, or religion (some have argued that Buddhism is more philosophy than religion anyway). They show up regularly in trauma work:
RAIN (Recognize, Allow, Investigate, Nurture) - a mindfulness practice for being with difficult emotions. Tara Brach has developed and popularized it; her guided RAIN meditations are free on her website and on Insight Timer.
Self-compassion practice - Kristin Neff's research and practices around self-compassion, which is particularly helpful when shame and self-criticism are loud (as they often are in CPTSD). Her practices are available on her website (self-compassion.org), on YouTube, and on Insight Timer.
Both have lineage in Buddhist contemplative traditions and stand on their own as practical, evidence-supported tools.
Treating sleep directly
Sleep often gets treated as a symptom that will resolve when the rest resolves. It usually doesn't. Treating sleep directly often makes everything else more workable, partly because sleep deprivation amplifies the autonomic activation that PTSD is already producing.
CBT-I (Cognitive Behavioral Therapy for Insomnia). The gold standard for chronic insomnia, with strong evidence in PTSD too. A specific protocol, around 6 to 8 sessions, distinct from general therapy. Worth asking for by name. Available via specialist clinicians and several validated apps (CBT-i Coach is free, made by the VA).
IRT (Imagery Rehearsal Therapy) for nightmares. You rewrite a recurring nightmare with a different ending and mentally rehearse the new version daily. Sounds odd, has surprisingly good evidence, dramatically underused. If nightmares are a feature of your sleep, this is worth doing. If you can't access an IRT-trained clinician immediately, guided IRT-style meditations exist on Insight Timer and YouTube as a starting place (they're not a substitute for working through it with a clinician, but they're a reasonable bridge).
A wind-down routine. This is underrated and gets skipped because it sounds simple. Anything you do consistently before sleep that signals "transition" to your nervous system helps. Can be short, longer, or elaborate:
Short (1-5 minutes, even in bed as you're falling asleep): a brief grounding practice, a few rounds of slow breathing, a body scan, gentle stretching.
Longer (20-40 minutes): a calming guided meditation or sleep hypnosis recording (Insight Timer is a deep library; many free options on YouTube), prayer, contemplative practice, journaling, reading something that isn't activating.
Elaborate (an hour or more): a warm bath with lavender oil (the post-bath core-temperature drop helps your body get ready for sleep), tea ritual, longer meditation, creative practice, gentle yoga.
The opposite is also true: watching a horror series or scrolling stressful news right before bed wires you for poor sleep. The point is intentionality - whatever you do, do something that tells your nervous system you're transitioning out of the day.
Medication options for sleep: prazosin (an alpha-1 blocker, used for nightmares - the large 2018 PACT trial in veterans was negative, which complicated the previously enthusiastic picture, but it still helps some people meaningfully); trazodone; hydroxyzine; mirtazapine; low-dose doxepin; melatonin. Each has its tradeoffs. None of them solve PTSD-related sleep on their own.
What to avoid for sleep: alcohol (very common as a sleep aid, makes sleep architecture worse, makes mornings worse, makes PTSD worse over time), and benzodiazepines or Z-drugs as ongoing solutions (effective short-term, problematic long-term, and they interfere with the extinction learning that trauma-focused therapy depends on).
A note worth knowing: sleep apnea. There's a substantial overlap between PTSD and obstructive sleep apnea (OSA). Studies in veteran populations have found OSA in 50-69% of those with PTSD (some series higher), and treating OSA - typically with CPAP, sometimes with an oral appliance - is associated with meaningful improvements in PTSD symptoms and nightmares in patients who use it consistently. The data is mostly from veterans and may not generalize as cleanly to all populations, but the principle holds: untreated OSA worsens both sleep and PTSD. If your sleep doesn't improve with the interventions above, or if you snore, wake up gasping, have unrefreshing sleep despite enough hours in bed, or have a partner who's noticed pauses in your breathing, worth asking about a sleep study. It's a fixable thing that gets missed.
Medication for the bigger picture
Medication is rarely sufficient alone for PTSD. It often helps make the other work possible - by taking the edge off panic, improving sleep, or stabilizing mood enough to engage in therapy. I think about it as a layer that supports the rest, not a layer that does the rest.
SSRIs. Sertraline and paroxetine are FDA-approved for PTSD. Effects are modest on average - they aren't miracle drugs - but for some people they meaningfully reduce hyperarousal, intrusive symptoms, and mood symptoms. Sertraline is usually my first try, given the side-effect profile and how well it tolerates dose adjustment.
SNRIs. Venlafaxine has reasonable evidence. Tends to be more activating, which can help when fatigue and shutdown are prominent and can be too much when panic and hyperarousal are.
Prazosin. Already covered above for nightmares. Worth a trial when nightmares are prominent; don't be disappointed if it doesn't do much for the rest of the picture.
Mirtazapine. Sedating antidepressant. Helps sleep and appetite. Useful when both are wrecked.
Topiramate, lamotrigine. Mixed evidence, sometimes used adjunctively for hyperarousal or comorbid mood symptoms.
Benzodiazepines. I'm going to be direct: the consistent finding in the literature is that benzodiazepines worsen long-term PTSD outcomes, even though they reduce panic in the moment. They interfere with the extinction learning that trauma processing depends on. If you've been on them, we can talk about it (the answer isn't always to stop immediately). I won't start them for PTSD.
What about ketamine, MDMA, psilocybin?
You may be hearing about these, or wondering. Here's an honest take.
Ketamine. FDA-approved for treatment-resistant depression (as esketamine/Spravato) and used off-label for PTSD. Effects can be rapid and meaningful for some people, transient for others. Ketamine-Assisted Psychotherapy (KAP) frames the medication experience as part of a larger therapeutic process, which is closer to how I think this work is best done.
A few things I'd add if you're considering it. Work with someone who has trauma training, not just someone administering ketamine. Look for a "low and slow" (psycholytic) starting approach - sub-psychedelic or lightly psychedelic doses that let you build trust with the therapist and with the medicine before going deeper. Higher doses can come later, when there's enough container for them. The relational quality of the work matters as much as the molecule. It's not for everyone, and it isn't a shortcut around the other work.
MDMA-assisted therapy. Of the psychedelic-assisted approaches, MDMA-AT looks most promising for trauma specifically. The mechanism makes sense: MDMA appears to resource the person (via oxytocin, reduced amygdala reactivity, increased empathy and trust) while they contact difficult material. That combination - safe enough to approach the hard thing - is exactly what trauma processing needs.
There's also an interesting body of work from Gül Dölen's lab (Nardou et al., Nature, 2019 and 2023) showing that MDMA temporarily reopens a "critical period" for social reward learning in mice - a developmental window during which the brain is unusually receptive to learning the meaning of social experiences. The window normally closes after adolescence. The 2023 follow-up showed similar effects for ketamine, psilocybin, LSD, and ibogaine, with different durations of openness. The proposed implication for PTSD is striking: MDMA may not just help process the original memory, it may briefly reopen the kind of neural plasticity that allows new social and safety learning to be encoded in the place where the old learning got stuck. Mouse research doesn't translate directly to humans, but it offers a candidate mechanism that fits the clinical observations.
Phase 3 trials (Mitchell et al., Nature Medicine, 2021 and 2023) showed strong efficacy signals for PTSD. The FDA declined approval in August 2024. The agency released its full Complete Response Letter publicly in September 2025, citing concerns about blinding, durability data, and safety reporting, and an additional Phase 3 trial has been requested. As of now (2026), MDMA-assisted therapy is not legally available in formal medical settings in the U.S. The research is ongoing; a timeline for any approval is not predictable.
Psilocybin. Oregon has a legal supervised-use model (not medical treatment - that distinction matters), and Colorado is rolling out a similar model. Federally still illegal. PTSD evidence is preliminary: small open-label studies, case series, ongoing trials.
Other psychedelics (psilocybin, ayahuasca, ibogaine, others) have been hypothesized to help with trauma based on various theoretical mechanisms, but the research is much less developed than for MDMA-AT specifically. Worth treating as "interesting and worth watching" rather than "established options."
My orientation: these can be valuable in the right context, with thorough preparation and integration, for the right people. They are not better than trauma-focused therapy. They are sometimes a useful additional tool, especially when more standard treatments have been tried. The cultural conversation often outruns the evidence; I try not to let either over-enthusiasm or dismissal close the conversation off.
Stellate ganglion block (SGB)
Worth its own section because it doesn't fit neatly into the other categories. SGB is a procedure - not a medication, not psychotherapy - in which a local anesthetic (typically bupivacaine or ropivacaine) is injected near the stellate ganglion in the neck, which is part of the cervical sympathetic chain. The hypothesis is that briefly interrupting sympathetic nervous system activity can recalibrate the hyperarousal of PTSD.
The evidence base is real and growing, mostly in military and veteran populations:
Hanling et al. 2016 (Regional Anesthesia and Pain Medicine) - a randomized, double-blind, sham-controlled trial showing meaningful PTSD symptom reduction with SGB.
Mulvaney et al. 2014 (Military Medicine) - case series of 166 service members with combat-related PTSD, positive outcomes.
A more recent RCT analyzed by Blakey and colleagues in 2024 (Translational Psychiatry) - the strongest effects were on the arousal and reactivity symptom cluster, which fits the proposed autonomic mechanism.
A 2025 systematic review and meta-analysis (Autonomic Neuroscience) - supportive overall, while noting the total body of evidence is still small.
What to know if you're considering it. Effect can be rapid - sometimes within hours to days. Duration is variable, often weeks to months; some people need repeat blocks to sustain the effect. The procedure itself is brief (15 to 30 minutes, ultrasound-guided), performed by anesthesiologists or interventional pain specialists. Side effects are usually mild and temporary (Horner's syndrome - droopy eyelid, small pupil, flushed face on the side of the block - resolving as the anesthetic wears off). Serious complications are rare in experienced hands.
The honest picture: SGB isn't a replacement for trauma-focused therapy. The autonomic effect appears real and is sometimes substantial; the effect on the deeper memory and meaning layer is less established. Some people use SGB to lower autonomic load enough to actually engage in therapy, which is a defensible strategy.
Access: most readily available at military and VA-affiliated programs, and at specialty pain or anesthesia clinics that have developed an SGB practice. Cost varies; sometimes covered by insurance, often not. Worth asking about if hyperarousal is the dominant feature for you and you haven't responded to other autonomic-targeted interventions.
Supplements and adjuncts
Worth knowing about, with appropriate expectations.
Most supplements don't have strong RCT evidence specifically for PTSD. Some have decent evidence for related symptoms (anxiety, sleep, depression). Some have plausible mechanisms and consistent positive anecdotal reports. None of these replace the other layers of treatment; they can be useful as adjuncts, particularly for the autonomic and sleep layers. If you're cautious about prescription medications, some of these (lavender oil especially, with actual anxiety RCT data) function as reasonable first-line options on their own, not just supplementary.
Listed roughly in order of evidence strength for anxiety and related symptoms:
Lavender oil (CalmAid). A standardized lavender preparation - essentially concentrated lavender essential oil in a pill - with anxiety RCT data that's more substantial than most supplements can claim. CalmAid is the accessible US version, available at drugstores and on Amazon (same active ingredient as Silexan, sold as a prescription product in Germany).
Here's what makes it worth knowing about. Kasper and colleagues ran a randomized, double-blind, head-to-head trial published in 2014 (International Journal of Neuropsychopharmacology): 539 adults with generalized anxiety disorder, comparing two doses of Silexan against paroxetine (an FDA-approved SSRI for GAD) and placebo over 10 weeks. Hamilton Anxiety Scale reductions were 14.1 points for Silexan 160 mg, 12.8 points for Silexan 80 mg, 11.3 points for paroxetine 20 mg, and 9.5 points for placebo. Both Silexan doses were statistically superior to placebo (p<0.01); paroxetine, in that trial, only showed a trend toward significance versus placebo. Response rates (≥50% HAMA reduction) were 60% for Silexan 160 mg, 52% for the 80 mg dose, 43% for paroxetine, 38% for placebo.
The safety profile is unusually clean for something with this much effect. Worst side effect in trials: lavender burps (eructation - basically tasting lavender for a bit after you take it). Not sedating. Not addictive. No tolerance buildup. No withdrawal - you can stop anytime without tapering. No significant drug interactions in the data so far. Each of those features is meaningful on its own; the combination is rare in anxiolytic options.
A word on the essential oil: you can't just buy a bottle of lavender essential oil from a health store and swallow some. Essential oils sold for aromatherapy aren't formulated for oral consumption, the concentrations are highly variable, and many essential oils on the market contain compounds that are unsafe to ingest. CalmAid/Silexan is a specifically standardized preparation - controlled active components, encapsulated for oral use, with contaminants tested for - in a defined dose. The plant matters; the preparation matters more.
Caveats worth holding alongside the evidence. This is for generalized anxiety disorder, not PTSD specifically. The trials have been sponsored by the Silexan manufacturer (Dr. Willmar Schwabe), which is a real source of potential bias even when the trial design is rigorous. A 2023 meta-analysis (European Archives of Psychiatry and Clinical Neuroscience) supported Silexan's anxiolytic effect across multiple trials, so the signal isn't from one study alone. None of this makes it a substitute for an SSRI when an SSRI is indicated. What it means: for the autonomic anxiety component of PTSD, if you're medication-wary, this is one of the strongest non-prescription options available, and the data behind it is unusually substantial for something that lives in the supplement aisle.
Ashwagandha (KSM-66 or Sensoril extracts have most of the data). Adaptogen with anxiety and stress RCT data (not PTSD-specific). Multiple trials, generally consistent positive signal. Generally well-tolerated. Caution with thyroid conditions, autoimmune disease, and pregnancy.
Saffron extract. Decent RCT data for depression; smaller data for anxiety and stress. Standardized extracts (Affron, Satiereal) have most of the evidence.
Inositol. Has RCT support for panic disorder specifically at higher doses (12-18 g/day), though dose-related GI side effects are common at those doses. Not PTSD-specific, but worth knowing about if panic is a prominent feature.
Magnesium glycinate (or threonate). Often rave-reviewed for sleep and nervous system regulation. Evidence for PTSD specifically is thin; broader anxiety and sleep data is modest but consistent. Reasonable to try; let me know if you have kidney issues.
L-theanine. Amino acid from green tea. Some anxiety and relaxation data, often used as a stimulant or SSRI adjunct. Low-risk; effects range from "noticeable calm" to "didn't do much" depending on the person.
Omega-3 EPA-dominant. Modest depression evidence; limited PTSD-specific data. Generally low-risk if you tolerate fish oil.
Cannabis and CBD. The picture is genuinely complicated. THC can reduce nightmares acutely for some people but has concerns about long-term PTSD outcomes (similar to benzodiazepines: short-term relief, worse trajectory in some studies; cannabis use disorder risk in regular users). CBD has cleaner but more limited data for anxiety. No real PTSD-specific RCT data for either. If you're using cannabis, worth being honest about how much, when, and why so we can think about it together.
A note on supplement quality: it varies dramatically. Look for third-party tested products (NSF, USP, ConsumerLab certified). Check with me before starting anything if you're on prescription medications - real interactions exist, especially with serotonergic agents, thyroid medications, and blood thinners.
Lifestyle infrastructure
The boring layer that holds everything else up.
Movement. Exercise has decent PTSD-specific evidence, both aerobic and resistance training. Doesn't need to be impressive. It needs to be regular. Three short walks beat one heroic gym session that doesn't repeat.
Alcohol. Often a quiet companion to PTSD. Worth being honest with yourself about. It disrupts sleep architecture, reduces SSRI effectiveness, and tends to make autonomic dysregulation worse over time. Reducing it (not necessarily to zero) often produces noticeable changes in sleep and reactivity within a couple of weeks.
Sleep regularity. More than total hours, consistent sleep and wake times stabilize the circadian system, which stabilizes mood and autonomic tone. Hard with PTSD. Worth the effort.
Nature exposure. Some evidence for nervous system effects of regular time outdoors. Lower bar than people think. Walking in a park counts.
Mind-body practice. Yoga, qigong, tai chi, structured breathwork. (Sudarshan Kriya Yoga, for example, has some PTSD-specific RCT data.) Pick one you'll actually do. Specificity matters less than regularity.
Community and connection
A category big enough to deserve its own section, especially for CPTSD or any trauma with a relational component. The opposite of trauma is connection, not relaxation.
Informal connection
The people whose presence regulates your nervous system. Friends who can sit with you when things are hard. Family members (chosen or biological) you can be honest with. Time with people who know you across years and don't need backstory. This category gets called "soft" or "supportive" but it's load-bearing.
Two different functions live here, and both matter:
Being seen. Telling your story, even in pieces, to someone who hears it without trying to fix it. This is where shame loosens. Where the compartmentalized parts get to come out into the light.
Just being yourself, doing things you enjoy. Time with people that has nothing to do with the trauma - where you're not "the person who went through that," you're just you, eating dinner, laughing at something, playing a game. This is where identity that isn't trauma gets built or rebuilt.
Both matter. Some people overweight the first and never get to the second; some never approach the first and stay isolated in the second.
Worth being intentional about nurturing the relationships that do this work for you. They're not automatic, and they atrophy without attention.
Formal support
Trauma support groups, CPTSD groups, harassment-specific groups, 12-step (for substance components), grief groups. These can be:
Peer-led (people who've been through similar experiences, no clinician)
Clinician-facilitated (often more structured, skills-oriented)
Online or in person - both have their place; in-person tends to deliver more nervous system co-regulation, online tends to be more accessible
A note worth knowing: support groups can be capacity-building or they can be primarily venting spaces. Both have value; they do different things. If you've been in a group where everyone is processing pain but no one is moving, it's not a flaw of the group - it's just one mode. Pairing that kind of space with practice-oriented work (somatic, skills, therapy) tends to move things forward.
Couples or conjoint therapy when relationships are affected
Cognitive Behavioral Conjoint Therapy for PTSD (CBCT, developed by Candice Monson and Steffany Fredman) has good RCT support for both PTSD symptoms and relationship outcomes when trauma is significantly affecting a partnership. Structured 15-session protocol that involves your partner directly in the trauma processing work, rather than running individual and couples therapy in parallel.
Finding a CBCT-trained clinician can be hard - it's not widely disseminated, and most couples therapists don't have specific PTSD training. The PTSD specialty programs at some academic centers and VA sites are the most likely places to find it. The principle (involving the partner directly in the trauma work) is sound and worth asking about even if formal CBCT isn't available, since some trauma-trained therapists are willing to do conjoint sessions in a similar structure.
Live somatic work with another person
Whether through a body-based therapist, group somatic practice, contact improvisation, partner yoga, or trauma-informed bodywork - presence with another regulated human is one of the most direct ways the nervous system learns that contact and safety can coexist. Especially powerful when the trauma was relational.
Spiritual, cultural, and meaning-making
PTSD often disrupts more than memory and physiology. It shakes your sense of safety, of self, of meaning, of where you fit in the world. Treating PTSD without acknowledging this layer can feel hollow - you can be less symptomatic and still feel like something is wrong about the world or about you.
This is where spiritual, religious, and cultural practices live. Some categories worth knowing about.
Religious and spiritual practice from your own tradition
Personal practice - prayer, meditation, contemplative practice, reading, ritual, the daily and weekly rhythms of your tradition. Doing your tradition's practices on your own.
Community and group engagement - services, study groups, retreats, holidays, the relational fabric of religious community. Showing up to be with people in shared practice.
Pastoral counseling - meeting with clergy (pastor, priest, minister, rabbi, imam, monk, etc.) for spiritual support around what you're going through. A real category of help, with one important caveat: clergy are not necessarily trained in mental health or trauma. Some are exceptional and trauma-aware; some can do harm by spiritualizing things that need clinical attention. Worth asking up front what kind of training and orientation the person has.
Religion-specific trauma frameworks and integrated therapies - several traditions have developed specific trauma-healing approaches: Christian-integrated psychotherapy and trauma-informed pastoral care; Jewish spiritual direction (hashpa'ah) and post-Holocaust trauma frameworks; Buddhist-informed therapy approaches and mindfulness-based trauma recovery work; Islamic counseling that integrates Quranic frameworks. Worth seeking out if you'd like to connect with these aspects of your religion as part of the healing.
For some people, religious community is also where harm happened (spiritual abuse, religious community siding with the harmer, traumatic experiences within the tradition). In that case this layer is more complicated and may need its own healing work - sometimes involving a different community, a different relationship to the tradition, or working with a therapist who specializes in religious trauma.
Spiritual practice not tied to a particular tradition
Meditation, contemplative practice, time in nature as a spiritual experience, mindfulness, secular Buddhist practice, the kind of philosophical engagement with mortality and meaning that some people find in writing, art, or solitude. Doesn't require you to sign on to any particular belief system.
Two Buddhist-influenced practices belong here too, since they're accessible without requiring commitment to a particular ideology or belief system: RAIN (covered under skills-based approaches above) and Kristin Neff's self-compassion work. Both have lineage in contemplative traditions but stand on their own as practical tools, and both have helped many people working through trauma, particularly with shame and self-criticism.
Group singing, kirtan, and the voice as practice. Worth a note of its own. Singing - especially sustained, group, or call-and-response singing - activates the vagus nerve directly through prolonged exhalation, vibration in the throat and chest, and (in group settings) co-regulation with other people doing the same thing. The autonomic effect is real and measurable, and the social effect of doing it with others is its own healing layer.
Kirtan is the call-and-response devotional singing rooted in Hindu and Sikh traditions, often part of the broader bhakti yoga lineage (the devotional branch of yoga that uses music, mantra, and intentional engagement to connect with the spiritual). It's widely practiced now in yoga and meditation communities and can be a real place to feel held, resourced, and in connection with something larger than yourself. On the appropriation question that comes up around practices that have crossed cultural lines: don't be overly scared off. The honest path is awareness and attribution - know the lineage, find local events with teachers who hold the practice with reverence, enjoy it.
One thing worth tracking with any spiritual practice, kirtan or otherwise: practice that supports and resources you for the rest of the work feels different from practice that's becoming a way to escape from feeling what you actually need to feel. (John Welwood named this drift "spiritual bypassing" back in the 1980s; it's a recognized pattern.) If you notice you're using kirtan or any contemplative practice to avoid hard feelings rather than to be more present with them, that's information worth holding. Both can happen at different times in different seasons; the practice itself isn't the problem, the relationship to it is.
Secular options are out there too: community choirs, sing-along events and movies, congregational singing if you have a religious community, group humming or toning practices, even singing in the car. The practice doesn't need to be sophisticated to do its work on the nervous system. Humming counts. Chanting counts. Singing along to something that names what you're feeling counts.
Cultural healing practices
Many cultures have developed their own trauma-healing frameworks over centuries or millennia. A non-exhaustive list of examples:
Native American and Indigenous North American: sweat lodges, talking circles, smudging, drum circles, the role of elders and ceremonial keepers (some practices in this tradition are considered sacred and closed to outsiders; if you're drawn to this work and aren't from these communities, working with Indigenous teachers who explicitly teach across cultural lines is the right path)
Mexican and Latin American: curanderismo, limpias (energetic cleansings), use of plants like copal, ruda, sage; community altars and ancestor practices
Korean: shamanic ritual (mudang/musok), processing of han (the accumulated grief and unresolved feeling that's a recognized cultural concept in Korea) through art, music, and ritual
Japanese: morita therapy (a structured psychotherapy founded by Shoma Morita in the early 20th century), naikan reflection (a structured contemplation of relationships developed by Yoshimoto Ishin)
Chinese: traditional Chinese medicine including acupuncture, herbalism, qigong, tai chi, ancestor practices
European folk traditions: regional practices vary widely and include Irish keening (ritualized mourning) and sean-nós singing; British and Celtic folk healing, herbal traditions, and seasonal/agricultural ritual; Spanish and Portuguese fado and cante jondo (deeply cathartic vocal traditions); Italian tarantella (a ritual dance historically associated with emotional and spiritual healing) and Marian processions; French pilgrimage traditions (Lourdes and others); Romanian descântec (incantation/charm traditions practiced by folk healers), călușari (a ritual brotherhood with healing dances), and bocet (ritual lament); Dutch and Northern European folk medicine; Russian Orthodox spiritual practices, banya (the steam bath as ritual cleansing), and folk healers (znakhar); Saami practices in Scandinavia; pan-Slavic and pan-European mourning practices and herbal traditions
African and African diaspora: traditional practices vary by region - sangoma in southern Africa, Yoruba and Ifá traditions in West Africa, drum and rhythm-based work, ancestral connection practices; in the diaspora, candomblé, santería, and various community-based healing traditions
Buddhist and Hindu traditional contexts: meditation, mantra, kirtan, ayurvedic frameworks that integrate trauma understanding with physical health
If a tradition is part of your cultural background, returning to it can be powerful. If it's not, approach with humility: there are real questions about appropriation, and there are also legitimate non-Indigenous teachers (and Indigenous teachers who teach across cultural lines) working in this space. The integrity of the practice, the credentials and lineage of the teacher, and the quality of the relationships involved matter more than cultural origin per se.
Soul retrieval and parts-based spiritual frames
Many traditions describe trauma as a loss or fragmentation of self - parts of you that left during the experience and need to be invited back. This frame maps interestingly onto contemporary parts work like IFS, though the language, ritual structure, and theory are different. For some people, the spiritual framing reaches something the psychological framing doesn't.
If you're drawn to this and want to explore: you'd look for a soul retrieval practitioner or a shamanic practitioner. The Foundation for Shamanic Studies and the Society for Shamanic Practice maintain practitioner directories. Sandra Ingerman's books and trainings are widely respected in the contemporary shamanic field. As always, credentials, lineage, and personal fit matter; trust your gut about a practitioner the same way you would with a therapist.
Plant medicine traditions
Touched on earlier with KAP and psilocybin. Worth flagging again that traditional ceremonial use of plant medicines (ayahuasca, peyote, psilocybin mushrooms, others) sits at the intersection of spiritual practice and trauma healing. Different context, ethics, and risks than medicalized KAP. Worth knowing about; not a starting point.
I don't push any particular framework. Attention to this layer tends to matter for full recovery, especially for trauma that disrupted meaning and identity. It's often the work that gets fuller attention later in treatment, once the acute layers have settled enough to allow it. Worth holding alongside the rest.
Books and resources
A curated starting list. Not exhaustive.
For understanding trauma
The Body Keeps the Score by Bessel van der Kolk - the dominant trauma overview book of the last decade. Comprehensive, readable, integrates neuroscience with clinical examples. Long. Worth it.
The Biology of Trauma by Aimie Apigian (2025, foreword by Gabor Maté) - newer, focuses on the cellular and physiological side of trauma. Good companion to van der Kolk if the body and biology angle interests you.
The Myth of Normal by Gabor Maté - broader sociocultural take on stress, illness, trauma, and modern life. Heavier on culture than clinical specifics.
What Happened to You? by Bruce Perry and Oprah Winfrey - childhood trauma and how early experiences show up in adult life. Accessible, conversational format. Good entry point if van der Kolk feels intimidating, especially if your trauma history is developmental.
For complex / developmental trauma specifically
Complex PTSD: From Surviving to Thriving by Pete Walker - probably the most useful CPTSD book for laypeople. Walker is both a survivor and a clinician, and it shows.
Holistically Treating Complex PTSD: A Six-Dimensional Approach by Pete Walker - his more recent book; written for therapists, coaches, and helpers more than for laypeople, but valuable if you're working through CPTSD and want depth (or if you want to share the framework with your therapist).
For inner work and parts-based approaches
No Bad Parts by Richard Schwartz - introduction to IFS from its developer. Accessible.
How to Do the Work by Nicole LePera - practical, sometimes oversimplified, but useful for daily practice orientation.
Apps
A curated list. The ones I recommend earn their place either by being free and evidence-based, or by doing one specific thing well that other apps don't.
For acute panic specifically:
Rootd - the "Rootr" button gives step-by-step guidance during a panic attack; includes breathing tools and journaling. Designed specifically for panic. Helpful when you need something concrete in the moment.
DARE Anxiety Relief - based on Barry McDonagh's "DARE response" approach, which teaches you to stop fighting anxiety and instead accept and move through it. The approach has loyal users and a real framework behind it.
For PTSD-specific coping:
PTSD Coach - developed by the U.S. Department of Veterans Affairs, free. Provides psychoeducation, symptom tracking, and coping exercises. Useful for non-veterans too despite the name.
For anxiety and CBT skills:
MindShift CBT - free, from Anxiety Canada. Uses CBT framework to teach strategies for worry, panic, perfectionism, social anxiety. Solid bones, no upsell.
For meditation, sleep, and broader practice:
Insight Timer - free, deep library of guided meditations, sleep meditations, IRT-style nightmare work, trauma-informed practices. Paid courses available too. The single most useful general app on this list.
For specific protocols:
CBT-i Coach - free app from the VA for CBT-I.
Breathwrk - structured breathing exercises (also mentioned under right-now tools as a breath pacer).
A note on the broader wellness apps (Calm, Headspace): they have decent meditation content but aren't trauma-specific. Fine to use, not substitutes for trauma-focused care. Sanvello, Panic Relief, and similar offerings are reasonable but don't add much beyond what the apps above already do well.
Online courses and free resources
The landscape is large and quality varies widely. A few starting points:
Tara Brach (tarabrach.com) - guided meditations including RAIN practice. Free on her website and on Insight Timer. Particularly useful for working with difficult emotions and the shame/self-criticism patterns common in CPTSD.
Kristin Neff (self-compassion.org) - research-based self-compassion practices and guided meditations. Free on her website and on Insight Timer. Important resource for shame work.
Pete Walker's website (pete-walker.com) - free articles and a CPTSD self-test that many people find clarifying.
IFS Institute (ifs-institute.com) - introductory courses and a trained-practitioner directory.
EMDRIA (emdria.org) - Eye Movement Desensitization and Reprocessing International Association maintains a directory of EMDR-trained therapists, searchable by location and specialty.
Bessel van der Kolk's online trauma courses are available through various platforms.
Free content on YouTube and elsewhere is plentiful but variable - some excellent, some misleading. For specific recommendations based on what you're working on, bring it up in session.
A note: no book or app substitutes for live work. Reading about trauma can be both helpful (understanding, framing, validation) and a trap (intellectualizing instead of feeling). If you find yourself reading more than practicing, that's a signal.
Notes on the evidence
PTSD treatment is genuinely better-evidenced than some psychiatric conditions, and the popular conversation around it varies in accuracy. A few things worth knowing as you choose what to try:
The trauma-focused psychotherapies (CPT, PE, EMDR, Written Exposure) have the most accumulated research. If you haven't done one, the question of whether to is meaningful.
SSRIs help modestly on average. They aren't transformative for most people, but they help some, and they make other work easier for many. Worth a trial if symptoms are significant.
Brainspotting and somatic approaches have a thinner research base than the trauma-focused therapies, partly because they're newer, partly because they're harder to study in RCT designs. Plenty of people find them genuinely useful in practice. Worth considering based on fit.
IFS and DBT skills have growing research bases. DBT skills are well-established for emotion regulation broadly; IFS-specific PTSD trials are smaller and more recent but converging on positive signals.
Psychedelic treatments are an active research area; MDMA-AT has the strongest signal so far for trauma specifically. The cultural conversation often outruns the data.
Supplements vary - some have decent evidence for related symptoms (anxiety, sleep, depression), most don't have direct PTSD evidence. Useful as adjuncts with appropriate expectations.
The integrative frame doesn't mean every option is equally good. It means we use multiple layers because PTSD lives in multiple layers - and we still weigh evidence, side effects, fit, cost, and access. I try to be honest about what we know, what's emerging, and what's plausible but not yet supported.
What to bring when discussingn with your clinician:
It helps us to know:
What you've already tried (therapies, medications, body work, supplements, anything) and how it went
What you're most miserable about right now - panic, sleep, intrusive memories, avoidance, numbness, dissociation, irritability, something else
What you're afraid of - in treatment, in yourself, in the process
How alcohol, cannabis, or other substances factor in (no judgment, real information)
What kind of work you're drawn to (talk, body, medication, group, plant medicine, skills, spiritual practice)
What's working - what's holding you up, what helps you settle, who's safe
A sense of your trauma history if you're willing - whether it was a discrete event, a series, or ongoing/developmental, because that shapes the plan
Whether you're still in the environment where the trauma happened, or have left
Who knew, and how they responded - because the response shapes the picture as much as the event
Whether identity-affirming care matters to you in finding referrals or adjuncts - LGBTQ+, BIPOC, neurodivergent, religious, disability - some people find this essential, others find it irrelevant, and either is valid; it just helps me point you in useful directions
The goal isn't to do everything on this menu. It's to find the two or three layers that fit your life, your history, and what you can actually engage with right now. Treatment is iterative. We adjust as we go.
Also, you are not broken. You are already whole and always were whole - we’re just remembering that and clearing blocks clouding that.
Patricia Pop, MD · Stanford-trained, board-certified psychiatrist · patriciapopmd.com
This guide is educational and not a substitute for individual clinical care. If you are in crisis, call or text 988 (Suicide & Crisis Lifeline) or go to the nearest emergency room.