
Iboga Microdosing: A Reference Guide
Companion to: "The Wooden Mirror: What a Psychiatrist Found Inside an Iboga Microdosing Container"
Reviewed by Patricia Pop, MD - Board-Certified Psychiatrist
Last updated: March 2026
This reference guide is for educational purposes only. Ibogaine is classified as a Schedule I controlled substance in the United States. Nothing here constitutes medical advice, a treatment recommendation, or an endorsement of any illegal activity. Anyone considering work with iboga should do so only within legal frameworks and with appropriate medical supervision.
What is iboga?
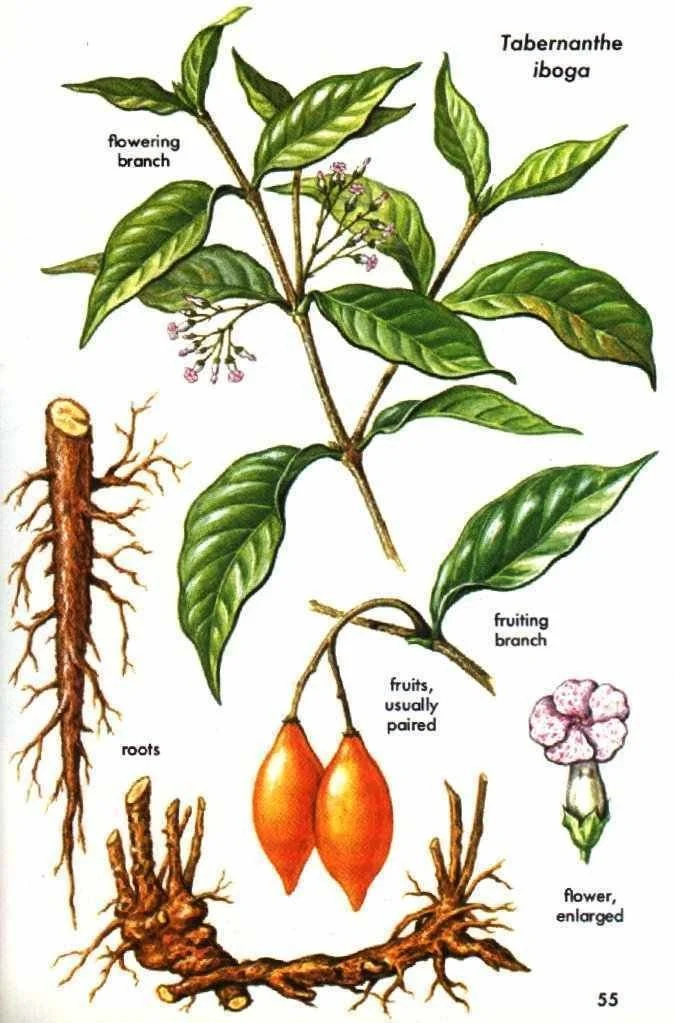
Iboga (Tabernanthe iboga) is a perennial rainforest shrub native to West Central Africa, primarily Gabon, Cameroon, and the Congo Basin. The root bark contains over 30 alkaloids.
The most studied is ibogaine, but others include ibogamine, ibogaline, tabernanthine, coronaridine, and voacangine. These alkaloids work together in whole root bark in ways that isolated ibogaine alone does not fully replicate.
Iboga has been used for centuries, possibly millennia, within the Bwiti spiritual tradition practiced by the Babongo, Mitsogho, Apindji, and Punu peoples of Central Africa. The Republic of Gabon declared iboga a national treasure in 2000.
Image: Alchetron.com
Iboga is classified as an "atypical psychedelic" or oneirogen (dream-producing substance).
Unlike classic psychedelics such as psilocybin or LSD, which primarily act on serotonin 5-HT2A receptors, ibogaine interacts with multiple neurotransmitter systems simultaneously.
The subjective experience is also distinct - practitioners consistently describe iboga as more introspective and self-reflective than visionary, sometimes compared to a waking dream state rather than the perceptual shifts associated with classic psychedelics.
Wait. What's an alkaloid?
You’ll hear a lot about these in the plant medicine space.
If you've had coffee, chocolate, or black pepper today, you've already consumed alkaloids. They're naturally occurring compounds that plants produce, often bitter-tasting, that happen to interact with our nervous systems. Caffeine is an alkaloid. So is nicotine. So is morphine. The word comes from "alkali" - they tend to be chemically basic (in terms of their pH, not their love of lattes and Ugg boots).
Iboga root bark contains over 30 different alkaloids, each with slightly different effects. That’s what makes it so hard to “isolate” one “active ingredient”. The effect is likely a symphony of all of them working together. This is sometimes described as an “entourage effect”.
Ibogaine is just one alkaloid of 30. It’s the most abundant and the most studied, but it's not the whole story. This is one reason whole root bark can produce somewhat different experiences from purified ibogaine-only. It’s similar to how drinking coffee and taking a caffeine pill aren't quite the same thing.
What is the difference between iboga, ibogaine, and noribogaine?
Iboga refers to the whole plant and, most commonly, to the raw root bark used in traditional practice. It contains the full spectrum of 30 (known) alkaloids.
Ibogaine is the primary psychoactive alkaloid extracted from iboga root bark (or semi-synthesized from voacangine, found in Voacanga africana). It is the compound used in most clinical research and in clinical treatment settings. Its half-life in humans is approximately 7 hours.
Noribogaine is ibogaine's primary metabolite, produced by the liver after ibogaine ingestion. It has a much longer half-life (24-50 hours) and acts primarily as a serotonin reuptake inhibitor and kappa-opioid receptor agonist. Noribogaine has been classified as a "psychoplastogen" - a compound that promotes structural and functional neural plasticity. The sustained presence of noribogaine is thought to be one reason ibogaine's effects persist well beyond the acute experience.
What is iboga microdosing?
Iboga is available in several preparations - whole root bark (used in traditional practice and most microdosing containers), total alkaloid extract (TA, a concentrated powder containing the full alkaloid spectrum), and isolated ibogaine hydrochloride (HCl, the isolated compound used in most clinical research and flood-dose treatment). These are not interchangeable.
Dosing differs significantly between forms, and the experience of whole bark versus isolated ibogaine is qualitatively (or “experientially”) different - similar to the difference between whole-plant cannabis and pure THC.
Most microdosing containers work with whole root bark and refer to it as “iboga”. If you encounter ibogaine HCl or TA extract, dosing guidance from someone experienced with that specific form is essential.
Microdosing iboga involves working with sub-perceptual to mildly perceptual doses of root bark on a cycling schedule. Typical parameters:
Dose range: 0.3 to 1.5 grams of root bark per session (or roughly 1-5 mg/kg ibogaine equivalent, though bark potency varies). That’s “about a pinky nail’s worth” (not an exact measurement, most of the time. Like the Italian “measure with your heart”).
Schedule: Commonly four days on, three days off, over a finite period of time (this should not be practicing ongoing)
Administration: In traditionally-informed containers, the bark is chewed (not capsulated), tucked into the cheek, and slowly chewed before swallowing. This allows sublingual absorption and brings the full sensory experience - taste, texture, the mild numbing - into awareness.
Timing: Morning dosing is most common (for its daytime clarity and focus). Some practitioners prefer late afternoon or evening, reporting that iboga activates dream life and has a more reflective quality at night. Experimentation is encouraged.
Food: One hour before and after dosing without solid food. Liquids are fine. Cacao (sometimes with adaptogenic mushrooms like reishi or chaga) in low doses are commonly used as a companion beverage.
In Bwiti tradition, this lower-dose practice is sometimes called the "hunter's dose," historically used for focus, energy, and stamina.
How does iboga microdosing differ from a flood dose?
Within the Bwiti tradition, these dose levels are not ranked hierarchically. They serve different purposes. Microdosing is its own practice, not a diluted version of the flood dose.
What do people report experiencing while microdosing iboga?
Reports vary widely. No two people describe the same experience, and individual sensitivity to iboga appears to be unusually variable. Experienced practitioners like Elizabeth Bast, co-founder of SoulCentro treatment center, report that some individuals have intense responses to doses that would be barely perceptible to others. This is why working within a guided container matters so much.
Some commonly described themes from practitioners and participants include:
Mild stimulant effect with increased energy and focus (the traditional "hunter's dose" effect). Some people describe this as “cleaner” or more sustained than caffeine.
Enhanced emotional access - crying unexpectedly, surfacing feelings that have been stored or avoided. "I didn't think anything happened. Then I sat down and cried for two hours."
Fatigue - which practitioners frame not as the medicine making you tired, but as it showing you where you already are tired. For people coming off caffeine or running on fumes, this can be pronounced.
Dream activation - more vivid, more narrative, more emotionally meaningful dreams, particularly with evening dosing.
Subtle shifts in habitual patterns - noticing your posture, your tone of voice, your reflexive reactions, as if from a slight distance. Not dramatic insight. More like a quiet "oh, I do that."
Nothing at all - some people, especially in the first week, genuinely notice nothing obvious. Practitioners consistently say this doesn't mean nothing is happening.
It is important to note: these are subjective reports, not clinical outcomes. Psychedelics are non-specific amplifiers, meaning they tend to amplify what's already present. Your experience in week one will likely differ from week four, and your experience will be different from anyone else's.
What does the on/off cycle actually feel like?
If this is your first time, your facilitator will likely tell you to consider starting on a day without major work or social obligations. Not because microdosing is incapacitating (it shouldn't be, at these doses), but because having open space lets you actually notice what's happening without having to perform normalcy at the same time.
Keep a journal. It doesn't have to be elaborate. Even a few words at the end of each day - on days and off days both. The shifts with iboga microdosing tend to be subtle enough that you won't always recognize them in real-time. You'll recognize them looking back or sharing. A journal is what makes that possible.
The off days are not empty days. Many people report that the second and third day of a microdosing cycle (the days immediately after dosing) carry their own quality - sometimes a subtle afterglow of clarity or emotional openness, sometimes a noticeable contrast that helps you see what the medicine was doing by its absence. Pay attention to the off days. They're part of the practice, not a gap in it.
Otherwise: live your normal life. The whole point of microdosing is that it integrates into your existing routine. You're not retreating from your life. You're paying closer attention to it.
How do you prepare for iboga microdosing?
Preparation is both practical and pharmacological.
Some of these are hard safety requirements. Others are strongly recommended practices within most containers.
Work with a clinician first. If you're on any psychiatric medications, cardiac medications, or other prescription drugs, talk to your prescriber before starting. Some medications require supervised tapering weeks or months in advance. Do not stop medications abruptly on your own. Use this as a general guideline, not for DIY.
Substances to stop or avoid (timeframes vary - discuss with your clinician and facilitator):
Because they inhibit CYP2D6 or CYP3A4 liver enzymes (slowing ibogaine metabolism, raising blood levels):
SSRIs: fluoxetine (Prozac), paroxetine (Paxil), sertraline (Zoloft)
SNRIs: duloxetine (Cymbalta)
Bupropion (Wellbutrin)
Grapefruit and grapefruit juice (inhibits CYP3A4 - the same reason it interacts with many medications)
St. John's Wort
Because they prolong QT interval (compounding ibogaine's cardiac effect on heart rhythm length):
Quinine, including tonic water (yes, really)
Certain antibiotics: azithromycin (Z-pack), fluoroquinolones
Certain antipsychotics: haloperidol, ziprasidone, quetiapine
Certain antiemetics: ondansetron (Zofran)
At iboga microdose levels the additive risk may be clinically negligible at standard doses, but worth asking about
Methadone
Because of serotonin syndrome risk:
SSRIs, SNRIs, MAOIs (overlap with above)
Tramadol
Triptans (migraine medications like sumatriptan)
5-HTP supplements
High-dose tryptophan supplements
Because of additive stimulant or cardiovascular effects:
Caffeine - including coffee, energy drinks, pre-workout supplements, matcha, and tea and green tea
Cocaine, amphetamines, MDMA
All stimulants including Adderall, Vyvanse, Ritalin, Concerta
Modafinil
Other substances most containers ask you to avoid:
Alcohol
Opioids (including kratom, which has opioid receptor activity)
Cannabis (some containers restrict this, others don't - ask your facilitator - but I would recommend avoiding)
Kava (liver metabolism concerns)
This list is not exhaustive. If you take any medication, supplement, or substance regularly, disclose it to both your clinician and your facilitator. The interaction profile of ibogaine is unusually broad. When in doubt, ask.
Baseline EKG. Required for flood dosing. If you have any personal or family history of heart rhythm issues, fainting, or sudden cardiac events, this is non-negotiable.
Practical preparation:
Clear your schedule on your first dosing day if possible - not because it's incapacitating, but so you can actually pay attention
Set up a journal or notes practice
If your container includes altar work, ritual, or intention-setting practices, take time to set that up before you start dosing
Sometimes small amounts of cacao are used if you'd like a companion beverage (some people use cacao with adaptogenic mushrooms like reishi or chaga as a coffee replacement during the process)
What does the research say?
Flood-dose evidence (strongest data)
The Stanford MISTIC study (Cherian et al., 2024, Nature Medicine) is the landmark study. Thirty Special Operations veterans with traumatic brain injuries received magnesium-ibogaine treatment at a clinic in Mexico. Results at one month post-treatment:
88% average reduction in PTSD symptoms
87% average reduction in depression symptoms
81% average reduction in anxiety symptoms
Disability scores dropped from 30.2 (moderate disability) to 5.1 (no disability)
Cognitive testing showed improvements in concentration, information processing, memory, and impulsivity
No serious cardiac events under the magnesium co-administration protocol
The full study, including outcome figures, is freely available: Cherian et al., 2024, Nature Medicine (ClinicalTrials.gov registration). For a more accessible summary, see Stanford Medicine's writeup.
A 2025 follow-up (published in Archives of Physical Medicine and Rehabilitation) found increased cortical thickness and a reduction in predicted brain age of 1.6 years one month after a single treatment.
Based on these findings, Texas committed $50 million to fund ibogaine clinical trials, and Arizona invested $5 million.
Important context: This was a prospective observational study, not a randomized controlled trial. The sample was small (n=30), all male, and all Special Operations veterans. Larger, controlled replications are needed.
Effect sizes this large in an uncontrolled study should be interpreted with caution - they may reflect placebo effects, the impact of traveling to Mexico for treatment, group bonding, complementary therapies provided alongside ibogaine, or genuine pharmacological effects. Likely some combination.
Neurobiology
Ibogaine has an unusually broad pharmacological profile, interacting with multiple neurotransmitter systems simultaneously:
Serotonin transporter (SERT): Both ibogaine and noribogaine inhibit serotonin reuptake, which may contribute to antidepressant effects.
Dopamine transporter (DAT): Modulation of dopamine systems is relevant to addiction and reward circuitry.
Opioid receptors (mu and kappa): Interaction with opioid receptors is thought to underlie ibogaine's ability to reduce withdrawal symptoms and cravings.
NMDA receptors: Antagonism at NMDA receptors may contribute to neuroprotective and neuroplastic effects.
Nicotinic acetylcholine receptors (alpha-3-beta-4): May play a role in effects on nicotine and stimulant dependence.
Animal studies demonstrate that ibogaine upregulates three key neurotrophic factors in brain regions involved in dopamine signaling, reward, and cognition:
GDNF (glial cell line-derived neurotrophic factor)
ibogaine is one of very few known compounds reported to stimulate GDNF release, which has generated research interest
BDNF (brain-derived neurotrophic factor) - more commonly stimulated by neuroplastic agents
NGF (nerve growth factor)
These neurotrophic factor changes were observed at higher doses (20-40 mg/kg in rats). Whether microdosing levels produce meaningful neurotrophic effects in humans is plausible, but yet unknown.
Microdosing evidence (very limited)
As of early 2026, there are no published randomized controlled trials of iboga microdosing for any indication (our system still thinks and categorizes research on DSM labels, HiTOP and RDOC tried to move us away from it - but it’s very much still there).
The published evidence consists of:
One case report (Fernandes-Nascimento et al., 2022, Brazilian Journal of Psychiatry): Ibogaine microdosing (4mg ibogaine HCl twice daily for 60 days) in a patient with bipolar type II depression. Progressive improvement in depression (90% reduction on BDI), anxiety (56% reduction on BAI), and hopelessness (100% reduction on BHS) scores, sustained 30 days after stopping.
Anecdotal reports from practitioners and participants.
Pharmacokinetic rationale: Periodic low doses may sustain noribogaine levels and extend the neuroplasticity window. Plausible but unconfirmed in human studies.
What are the safety considerations?
Cardiac risk
Ibogaine affects cardiac repolarization through hERG potassium channel blockade, which can prolong the QT interval. At flood doses, this has been associated with fatal cardiac arrhythmias. For those with pre-existing QT problems, heart rythym issues, or other QT-prolonging meds - this can be deadly. The vast majority of ibogaine-related deaths have occurred during detox procedures, but the cardiac mechanism is dose-dependent yet not completely absent at lower doses.
Baseline EKG is strongly recommended. It would be best and most prudent to obtain baseline EKGs even for microdosing, and I can imagine this becoming required if this enters common practice. However, it’s more often than for microdosing, participants will be asked about their medication and heart health history. This does have a chance of course, in missing omissions or simply those unaware of their pre existing heart problems. It’s what’s happening though, right now.
For flood dosing, EKG and continuous cardiac monitoring are required.
The Stanford MISTIC protocol used intravenous magnesium co-administration to mitigate cardiac risk, with no serious cardiac events reported.
Accumulation Risk:
An important pharmacokinetic note is that noribogaine, ibogaine's primary metabolite, has a long half-life (24-50 hours). With repeated dosing, noribogaine can accumulate. If you notice the effects becoming stronger at the same dose over successive days, this may indicate accumulation, and you should reduce your dose or extend your off days. This is one reason the cycling schedule (days on, days off) matters - it's not arbitrary. It's allowing clearance.
Drug interactions
Ibogaine is metabolized primarily by the CYP2D6 enzyme. Medications that inhibit CYP2D6 can dangerously slow ibogaine metabolism, raising blood levels:
SSRIs: Fluoxetine (Prozac), paroxetine (Paxil)
SNRIs: Duloxetine (Cymbalta)
Other: Bupropion (Wellbutrin), amitriptyline, quinidine, ritonavir, sertraline (Zoloft), terbinafine
Serotonin syndrome risk: Combining ibogaine with serotonergic medications (SSRIs, SNRIs, MAOIs, tramadol, triptans) can precipitate serotonin syndrome, a potentially life-threatening condition.
QT-prolonging medications: Combining ibogaine with other QT-prolonging drugs (certain antiarrhythmics, antipsychotics, some antibiotics) compounds cardiac risk.
Stimulants and caffeine: Most iboga protocols require abstinence from caffeine, as it can interact with the pharmacokinetics of iboga alkaloids and increase cardiovascular strain.
Bottom line: If you are considering iboga work at any dose level, you need a clinician involved in the decision-making. Don’t just self-check based on this guide alone. Tapering, also if appropriate, must be done carefully and with proper medical supervision.
Pregnancy, breastfeeding, & fertility
There is insufficient safety data. Avoid iboga during pregnancy and breastfeeding.
Iboga's effects on fertility are not well understood by modern medicine. Some traditional uses include it as an aphrodisiac and, reportedly, for treating infertility - though the specifics of that traditional use are not well-documented in the ethnobotanical literature available in English. This should not be taken as evidence of reproductive safety. Avoid iboga if you are pregnant, breastfeeding, or actively trying to conceive.
Sourcing
If you are obtaining iboga outside of an established container or retreat, sourcing is a genuine safety concern. Adulterated, mislabeled, or degraded products have been documented. Some material sold online as iboga has been found to contain the wrong plant species or contaminants. The quality and potency of root bark varies significantly depending on the age of the tree, growing conditions, and how it was harvested and stored. Working within an established container with known, trusted sourcing is strongly recommended over self-sourcing
Who should certainly NOT use iboga
Anyone with pre-existing cardiac conditions or QT prolongation
Anyone on medications that inhibit CYP2D6 or prolong QT interval (without proper medical taper and clearance)
Anyone on serotonergic medications without supervised discontinuation
Anyone with active psychosis or severe dissociative disorders (insufficient safety data)
Pregnant or breastfeeding individuals
Even if you do not have these conditions, it is still recommended to be very careful and thorough with your clinicians.
What is a "container" in this context?
In psychedelic and plant medicine work, a "container" refers to the intentional structure that holds the experience. This includes the physical setting, the facilitators, the group agreements, the dosing protocol, the integration practices, and the relational field created by participants showing up together with shared intention.
In traditional psychotherapy - we also have a “container”, whether that’s the weekly 50min visit, or the monthly 3 hour intensive.
A microdosing container typically involves:
A small to medium group (often 4-25 people)
Experienced facilitators who guide the process across multiple weeks
Weekly group calls for sharing, reflection, and guidance
A private communication channel for ongoing support between calls
Specific agreements about substances to avoid, commitment to the dosing schedule, and participation expectations
Integration practices: journaling, ritual, altar work, spoken intention, dream tracking
The container model is distinct from solo microdosing. The group reflection, witnessing, and shared accountability appear to be therapeutically significant - the group sharing process is where you can practice noticing and changing relating patterns (do you shy away, dominate space, never ask for help, check out?) as well as recognize shifts in others’ experience that they hadn't noticed on their own (“I didn’t think that was much but now that I hear someone else's story, I realize these subtleties are important”).
Legal status (2026)
United States: Ibogaine is classified as a Schedule I controlled substance under the Controlled Substances Act (since 1970). It is illegal to manufacture, distribute, or possess. No state has decriminalized ibogaine (unlike psilocybin in some jurisdictions). Texas and Arizona have funded research programs but have not changed the legal status.
Legal or unregulated: Mexico (unregulated, where most clinical treatment occurs), the Netherlands, Germany, Gabon, Costa Rica.
Prescription or controlled access: Brazil, Canada, South Africa, New Zealand, Australia.
Illegal: Belgium, France, Ireland, Israel, Italy, Norway, Sweden, Switzerland.
Clinical trials are underway or approved in several countries. In the U.S., Delix Therapeutics received a 2023 NIDA award to study a non-hallucinogenic ibogaine analog (DLX-007) for substance use disorders.
Sustainability and ethical sourcing
Iboga grows in a very limited geographic range and takes approximately 7-15 years to reach harvestable maturity. The entire root system is typically harvested, and the tree dies in the process.
As global demand increases - particularly for ibogaine extraction for addiction treatment - wild iboga populations in Gabon face significant supply pressure. Ethical considerations include:
Sourcing from managed farms rather than wild harvesting when possible
Supporting conservation and community initiatives in Gabon, Cameroon, and the Congo
Recognizing that increased microdosing demand adds to supply pressure
Awareness that the Bwiti tradition depends on continued access to iboga for its own ceremonial and spiritual practices
Some practitioners and researchers are exploring semi-synthesis of ibogaine from voacangine (found in Voacanga africana, a more abundant and renewable source) as an alternative
Want to add more?
If you're someone experienced in iboga or other plant medicines and you'd like to share information, updates, clarification, or other insights - please do!
If you're a clinician curious about iboga or psychedelic-assisted work, I'm always happy to connect.
Reach out through my collaboration page or email drpop@patriciapopmd.com.
References
Cherian KN, Keynan JN, Anker L, et al. Magnesium-ibogaine therapy in veterans with traumatic brain injuries. Nature Medicine. 2024;30(2):373-381.
Marton S, González B, Rodríguez-Bottero S, et al. Ibogaine administration modifies GDNF and BDNF expression in brain regions involved in mesocorticolimbic and nigral dopaminergic circuits. Frontiers in Pharmacology. 2019;10:193.
Fernandes-Nascimento MH, Viana-Ferreira K, Chaves BDR, Negrão AB, Wang YP. Ibogaine microdosing in a patient with bipolar depression: a case report. Brazilian Journal of Psychiatry. 2022;44(4):451-452.
Ly C, Greb AC, Cameron LP, et al. Psychedelics promote structural and functional neural plasticity. Cell Reports. 2018;23(11):3170-3182.
Noller GE, Frampton CM, Yazar-Klosinski B. Ibogaine treatment outcomes for opioid dependence from a twelve-month follow-up observational study. American Journal of Drug and Alcohol Abuse. 2018;44(1):37-46.
Dos Santos RG, Bouso JC, Hallak JEC. A systematic literature review of clinical trials and therapeutic applications of ibogaine. Journal of Substance Abuse Treatment. 2022;133:108545.
Changes in brain structure and age in veterans with TBI after treatment with magnesium-ibogaine. Archives of Physical Medicine and Rehabilitation. 2025.
Hello! I'm Patricia Pop, MD - a board-certified psychiatrist based in Half Moon Bay, California offering remote psychiatry and therapy throughout California.
I offer integrative psychotherapy and medication management for adults, including psychodynamic therapy, CBT, brainspotting, and low-dose ketamine-assisted psychotherapy (see ketamineprep.com for my preparation guide). I work at the intersection of evidence-based psychiatry and relational healing - including psychedelic and altered-state assisted modalities. I love to write about the places where clinical science and experiential wisdom meet. Visit patriciapopmd.com or book at pop.intakeq.com/booking.
This post is for educational purposes only. Ibogaine is a Schedule I controlled substance in the United States. Nothing here constitutes medical advice or an endorsement of any illegal activity